
By Castine A. Bernardy, Nicola M. Elardo, Alexa M. Trautz, and James P. Malley, Jr., Ph.D., Environmental Engineers, University of New Hampshire
Worldwide concern over the risk of contracting or spreading COVID-19 has sparked widespread interest in using UV devices for air and surface disinfection. The purpose of this article is to provide tips to the consumers and users of UV devices intended to inactivate air and surface pathogens. That market contains thousands of different products, with over 50 million UV products sold to consumers since March 2020. Unfortunately, these products lack uniform validation protocols, manufacturing specification, or guidelines. Therefore, consumers need to be informed before purchasing or using UV devices.
There are three types of UV light commonly discussed in disinfection. UV-A and B wavelengths come from the sun and reach the Earth. UV-C wavelengths vary from 200 to 280 nm and are emitted from these purchased UV devices.
Generally, the lower the wavelength, the greater the photon energy of the light that is being emitted by the device. This is important to note when discussing disinfection due to the sun, as UV-A and UV-B have longer wavelengths. While disinfection from the sun may be possible, the time required to achieve adequate disinfection from the sun is excessive and often results in desiccation of the pathogen before it is inactivated by the UV ray.
What you should know
Often the information provided by advertisements and many very brief user manuals for UV devices simplifies operations to talking about time, instead of dose. Dose is the measurement that is recommended by all UV professionals because time is not the most important factor. The effectiveness of any UV device or application depends upon at least four key factors: a) the irradiance or fluence rate of the light source at specific wavelength(s) emitted (some refer to this as intensity or strength of light, but those are vague, non-technical terms), b) the optical geometry of the UV device, or how it is to be applied, c) the type of organisms to be targeted, including their action spectra and what percent removal (or log inactivation), is desired and d) contact time. Of these lamp characteristics, optical geometry and organism characteristics are far more important than time.
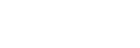
UV device geometry and optics matter when placing an object in it for disinfection, as shown in Figure 1. Figure 1 is a UV intensity “heat map” of a typical device disinfecting a KN95 mask (black). The heat map measures the sum of all optical factors that affect delivered UV dose, as confirmed by UV radiometer readings. The figure demonstrates that many regions of a typical UV device (blue) deliver a very low UV dose and will produce poor disinfection.
One way to determine if the UV device is effective at inactivating the pathogen of interest is by using UV dosimeter badges. UV dosimeter badges are reusable or single-use labels that change color as they receive UV radiation. When purchased, a pack of dosimeter badges will come with a color scale that matches each color to a UV dose. With this tool, the user visually can see if the required dose for disinfection has been achieved by matching their badge to the corresponding color on the scale after dosing. Thus, UV dosimeter badges offer consumers an easy way to confirm a UV device has done its job.
Safety concerns
Virtually all UV devices come with warnings about the potential electrical hazards and about the fact that UV light is known to cause harm to skin and eyes.
Dosing human and animal tissues with any forms of UV energy should not be done by the buyers and users of these UV devices. Special cases performed by experienced medical professionals under very tightly controlled conditions for very specific medical problems may be found in internet searches, but “do not do this at home” is the message for buyers and users of UV devices.
The current US and international guidelines set limits on maximum exposure to UV and highly recommend that living tissue should not be exposed to any forms of UV light unless it is prescribed and monitored by healthcare professionals.
Users must be vigilant to protect themselves from all direct, reflected or otherwise stray UV light when using any UV device, especially items such as UV wands.
In addition, ozone production is another potential hazard when operating enclosed UV devices. Normal use of UV devices for applying lower doses (0 to 100 mJ/cm2) to surfaces or air is being increased 10- to 20-fold (e.g., 2,000 mJ/cm2) to ensure PPE is adequately disinfected before reuse. The elevated doses may result in the unwanted generation of low levels of airborne ozone. Such ozone levels can cause minor irritation to the eyes, nose and throat, as well as low-grade headaches if people use these devices for extended periods of time.
In addition, the effectiveness of using UV wands is doubtful. Normal human limitations and error make it unlikely that consumers will hold the wand an appropriate distance from a surface, use the correct sweeping motion to cover the whole surface or expose the pathogen to a high enough UV dose to cause adequate inactivation.
Finally, it is extremely important to verify that you have purchased a quality UV device. Generally, the better-quality devices are hundreds to thousands of dollars and come with independent third-party testing data. However, price is not the only determinant for UV device excellence, and it is crucial to confirm that the UV device delivers the specified dose from the lamp by use of dosimeter badges. Finally, UV devices cannot replace the multiple barriers recommended by health experts to prevent the spread of diseases like COVID-19.
This article written under the supervision of Jim Malley, jim.malley@unh.edu. For more information on UV disinfection technologies, visit www.uvsolutionsmag.com.